This meta-analysis aims to investigate the impact of hypothermia on surgical outcomes in high-risk surgical patients. The study utilized databases including Google Scholar, MEDLINE, TÜRKMEDLINE, ULAKBİM, and CINAHL. A comprehensive search from January 2009 to May 2019 yielded 193 studies, with five meeting the inclusion criteria. Three independent authors conducted a quality assessment of the studies using established criteria, achieving a high inter-rater kappa agreement rate of 0.76. Two of the included studies were descriptive; the remaining were retrospective, retrospective cohort, and descriptive cross-sectional, respectively. The sample sizes ranged from 57 to 731, and none of the studies employed a standardized scale for evaluation. The evaluation of these studies indicates a negative impact of hypothermia on the surgical process, particularly in terms of recovery.
Introduction
A drop in body temperature below 36 °C is called hypothermia. Protective reflexes play a role in maintaining the body temperature in balance, but due to the decrease or disappearance of the reflexes due to anesthesia, the body temperature balance may not be maintained, and hypothermia occurs [1]. Hypothermia may develop in all patients during surgical processes [2]. Hypothermia is evaluated in three steps. These are the mild range, 34-36 °C; the medium range, 32-34 °C; and the severe range, less than 32 °C [3]. Hypothermia causes many risk factors in patients [4]. Among them, age, gender, body mass index, pre-existing low body temperature, unintended weight loss, chronic renal failure, duration and extent of surgery [4-6]. Hypothermia causes many complications. These wound infections increase in myocardial events, coagulopathy, sepsis, length of hospital stay, mortality, and prolongation of recovery [2, 7, 8].
While the management of hypothermia in surgical patients is so difficult, it is also a preventable condition [5]. Active and passive heating methods are used to prevent hypothermia. One or more radiation, conduction, and convection methods can be counted among the active heating methods. In order to provide this, hot air-blowing heating, electric blankets, radiant heaters, heat-moisture exchange filters, humidified and heated carbon dioxide are used. Passive heating methods are: The patient is protected against the cold from outside by materials such as blankets, socks, surgical drapes, piques, sheets, and clothes [9]. Efforts directed towards the prevention or management of hypothermia necessitate a thorough understanding of the clinical delineations of hypothermia and normothermia, the identification of risk factors contributing to hypothermia, discernment of adverse events linked to hypothermia, and the formulation of preventative strategies [1, 9, 10]. Based on all this information, it is extremely important to maintain normothermia, prevent complications due to hypothermia, and ensure patient safety. All health professionals are responsible for the management of this condition.
When the studies were examined, it was seen that there were no meta-analysis studies examining the effect of hypothermia on the surgical process. For this reason, this research will contribute both to care and to the literature.
Materials and Methods
Study objectives, design, setting, and duration
The primary objective of this investigation was to scrutinize the impact of hypothermia on the surgical process utilizing the meta-analysis methodology. The study spanned from January 2009 to May 2019.
Hypotheses
H1: The ambient temperature within the operating room significantly influences the occurrence of hypothermia.
Methodological approach
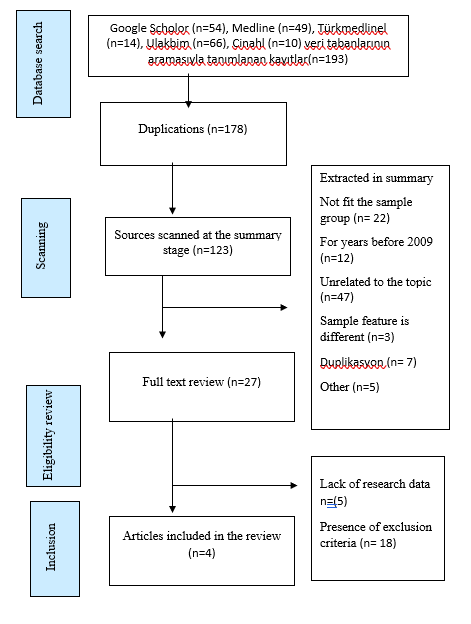
The procedures of this study were systematically organized according to the PRISMA (Systematic Reviews and Meta-Analyses Analysis Statement) [11] and MOOSE (Meta-Analyses of Observational Studies in Epidemiology) criteria described in the relevant literature. Articles meeting these criteria were identified and shown in Figure 1 and Table 1.
|
|
|
Figure 1. Prisma (Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement) |
Table 1. Moose (Meta-analysis of Observational Studies in Epidemiology)
|
Name of the study |
The authors of the study |
Year of Study |
Country |
Type of Study |
sample size |
Operating Room Temperature |
Quality evaluation score (A:9-12) (B:5-8) (C:1-4) |
|
Incidence of perioperative hypothermia in orthopedic surgery and risk factors |
Duman [12] |
2016 |
Türkiye |
cross-sectional |
116 |
× |
A |
|
Effect of hypothermia in patients undergoing simultaneous carotid endarterectomy and coronary artery bypass graft surgery |
Ozen [13] |
2015 |
Türkiye |
retrospective |
57 |
× |
A |
|
Survey on post-operative hypothermia incidence in operating theaters of Kocaeli University |
Aksu [14] |
2014 |
Türkiye |
Descriptive |
564 |
× |
A |
|
Cardiac surgery and local hypothermia: retrospective evaluation of the 731 patients |
Inan [15] |
2011 |
Türkiye |
retrospective |
731 |
× |
B |
Comprehensive literature review
The keywords for article searches were established by exploring the Turkish Science Terms database and medical topics using the MeSH Browser [16]. English equivalents of the identified terms, including "hypothermia," "low body temperature," "warming," "post-surgery," "post-operative," "perioperative," and "surgical patient," were employed for database searches. Relevant research articles published between January 2009 and May 2019 were sought using the keywords in Google Scholar, Medline, Türkmedline, Ulakbim, and Cinahl databases. A total of 193 articles were initially retrieved.
After eliminating duplicates and articles incongruent with title and abstract criteria, the remaining articles underwent further assessment through title and conceptual readings. Subsequently, articles suitable for full-text examination were identified, while those deemed irrelevant to the study topic were meticulously categorized and excluded. Data extracted from the selected studies adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement) [17] and MOOSE (Meta-analysis of Observational Studies in Epidemiology) criteria. This data encompassed study name, authors, publication year, country, study type, sample size, operating room temperature, and quality assessment score.
Search and meta-analysis criteria for articles
Inclusion Criteria and Methodological Quality Assessment:
The inclusion criteria for the study encompassed the following specifications:
Original, quantitative articles,
Articles written in both English and Turkish on the relevant subject,
Articles published in national/international refereed journals,
Studies incorporating patients with hypothermia,
Articles within the timeframe of the last decade (2009-2019),
Papers presenting a comprehensive quantification and thorough documentation of the total number of study groups and changes in primary outcomes (hypothermia and surgical patients),
Articles providing full-text access,
Exclusion of studies lacking validity and reliability assessments,
Omission of thesis studies, systematic reviews, and oral/poster presentations at congresses.
Methodological quality assessment involves a meticulous evaluation based on article review, coding, and adherence to inclusion criteria. Two independent researchers/experts conducted detailed abstract and full-text readings to mitigate publication bias. The coded information included descriptive features such as study title and authors, publication year and country, study type, sample size, operating room temperature, and quality evaluation score.
As proposed by Polit and Beck [18], Kappa statistics were employed along with 12 predetermined criteria for assessing research quality across all included studies. Each study underwent separate evaluation by researchers against all criteria, with a "1 point" awarded if a criterion was fully met and a "0 point" assigned if not. Studies meeting the inclusion criteria were then incorporated into the analysis. Quality categorization was based on the total points, with scores of 0-4 deemed poor, 5-9 considered medium, and 9-12 indicative of strong quality [17, 19]. The evaluation yielded scores ranging from 7 to 12, with a maximum score of 12 signifying good quality.
For the independent article selection and bias scoring conducted by three authors, inter-rater agreement was assessed using the Cohen kappa statistic. A kappa statistic between 0.41 and 0.60 was considered moderate, 0.61 and 0.80 were significant, and above 0.80 was regarded as perfect agreement. Utilizing the SPSS-25 program, the calculated kappa values for article-based evaluations were Cohen's kappa 0.76 within the 95% confidence interval (CI: 0.643-0.881). This study's overall agreement rate kappa value was determined to be 0.76, indicating high reliability.
Data analysis
Data was analyzed using the licensed "Comprehensive Meta-Analysis Academic/Non-profit Pricing (Version 3)" software. Information from all articles meeting the inclusion criteria and deemed suitable for inclusion in the study was entered into the CMA software. Cochran's Q statistics were employed to assess the heterogeneity among the articles. Heterogeneity, as measured by the I2 statistic, was categorized as follows: below 25% indicating non-existence, 25-50% denoting low, 51-75% signifying moderate, and over 75% representing high heterogeneity [20].
In the heterogeneity assessment, effect sizes, study weights, 95% confidence intervals, and the overall effect size of all studies were computed under the random effects model in group analyses with p ≤ 0.05 and under the fixed effects model in group analyses with p > 0.05. For binary data analyses, "RR and OR" values were the basis for assessing the overall effect size. The threshold for statistical significance in the comprehensive effect evaluation was set at p ≤ 0.05. Classic Fail-Safe N and Tau coefficient calculation results were utilized to test publication bias.
Results and Discussion
Research findings
The search yielded 193 studies, of which four met the inclusion criteria and were included in the study. Among these, two studies were retrospective, one was descriptive, and one was cross-sectional.
Evaluation of methodological quality
Kappa statistics proposed by Polit and Beck [18] and 12 predetermined criteria for research quality assessment were applied to all studies. Researchers independently evaluated each study on all criteria, receiving a "1 point" for fully meeting each criterion and a "0 point" otherwise. Articles meeting the inclusion criteria were categorized as poor quality with a total score of 0-4, medium quality with 5-9, and strong quality with 9-12 [20]. Following evaluation, the highest score among the studies was 9, and the lowest was 7. Three of the four studies (n=4) included in the study were rated as "strong," while one was rated as "moderate." All four studies meeting this criterion were included in the meta-analysis, as they were evaluated as moderate to strong quality. A table displaying the quality assessment of the four studies included in the meta-analysis, along with the distribution of scores in each domain, is presented in Table 1.
The Cohen kappa statistic assessed agreement between researchers for article selection and bias scoring. Using the SPSS-25 program, article-based kappa values were calculated within Cohen's kappa 95% confidence interval of 0.82 [Confidence Interval (CI) (CI: 0.724-0.921)]. Kappa values were interpreted as follows: < 0 indicating worse than random fit, 0.01 — 0.20 negligible agreement, 0.21 — 0.40 poor agreement, 0.41 — 0.60 moderate agreement, 0.61 — 0.80 good agreement, and 0.81 — 1.00 very good agreement [21], or 0.75 and above considered excellent, 0.40-0.75 moderate-good, and below 0.40 poor fit [21]. The obtained kappa value in this study indicates a very good agreement between the evaluators.
Effect sizes and heterogeneity
Operating room temperature, identified as a potential risk factor for hypothermia based on the findings of the studies, was designated as a covariate for all articles. Heterogeneity among studies was assessed using Cochran's Q statistic. The heterogeneity test results indicated a p-value less than 0.05, and the Q (15,862) value surpassed the value corresponding to the degrees of freedom, signifying a heterogeneous structure among the individual studies included in the meta-analysis. The I2 statistical value was computed as 81.087. Consequently, the effect size distribution was evaluated using the random effects model.
Table 2. Heterogeneity Test Results for the OR Temperature Variable
|
Model |
Effect size and %95 confidence interval |
Test of null (2-Tail) |
Heterogeneity |
|||||||||
|
Model |
Number Studies |
Point estimate |
Standard error |
Variance |
Lowe limit |
Uper limit |
Z-value |
P-value |
Q-value |
df(Q) |
P-value |
I-squared |
|
Fixed |
4 |
0,010 |
0,054 |
0,003 |
-0,095 |
0,116 |
0,186 |
0,853 |
15,852 |
3 |
0,001 |
81,087 |
|
Random |
4 |
-0,055 |
0,147 |
0,022 |
-0,344 |
0,234 |
-0,374 |
0,708 |
|
|
|
|
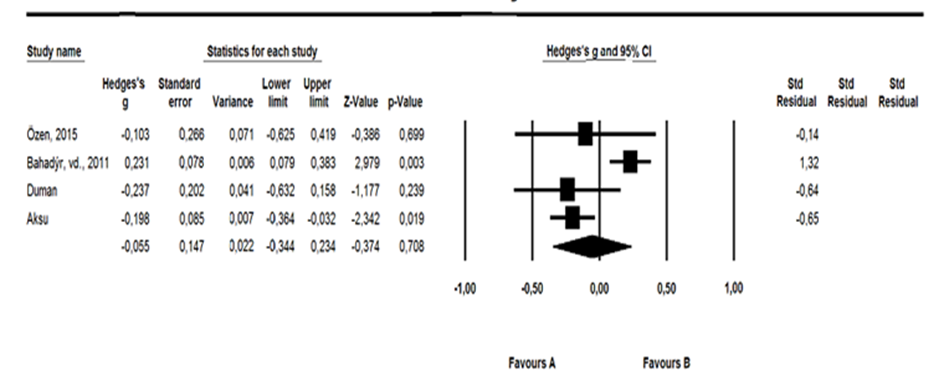
Analysis conducted utilizing the random effects model revealed that the overall effect size of operating room temperature on hypothermia exhibited a non-significant effect, as indicated by a value of 0.055 (95% Confidence Interval; -0.344 to 0.234; p < 0.05).
|
|
|
Figure 2. Meta-Analysis Diagram Showing the Impact Direction of the Study for Operating Room Temperature |
Publication bias
Kendall's tau b coefficient was calculated as another measure of the meta-analysis dataset to assess the probability of publication bias. In the absence of publication bias, this coefficient is anticipated to approach 1, and the double-tailed p-value will not be statistically significant, i.e., greater than 0.05 [22]. According to the calculated values (Kendall's tau b = 0.0628; p = 0.432), no evidence of publication bias was identified in the studies included in the meta-analysis.
Maintaining normothermia in post-surgical processes constitutes a critical parameter for recovery [23, 24]. Notably, the systematic review and meta-analysis by Lee and Kim in 2021 [25], focusing on the optimal application results of air heating to prevent perioperative hypothermia during abdominal surgery, demonstrated statistically significant findings. Similarly, the 2020 meta-analysis by Xu et al. [26]. suggested that the risks of hypothermia during surgery are lower than those reported in the literature. Another meta-analysis by Xu et al. in 2021 [27] concluded that hypothermia negatively affects the surgical process, leading to complications such as bleeding, surgical site infection, and shivering, compared to normothermia. In contrast, the 2019 systematic review and meta-analysis by Bu et al. [28]. found no association between perioperative hypothermia and surgical site infection. Results from Liu et al. 2019 systematic review and meta-analysis were consistent with the existing literature [29].
When independently evaluating the studies included in this analysis, it was observed that operating room temperature had a detrimental effect on the surgical process. However, upon aggregating the analysis results of all studies in this systematic review and meta-analysis, it was concluded that operating room temperature had no discernible impact on the hypothermia or overall surgical process [30]. This observation is attributed to the limited number of studies available in the literature.
Conclusion
Based on our research findings, the examination of hypothermia's effect on the surgical process suggests that both the high incidence of hypothermia and inadequate warming practices during surgery may contribute to suboptimal patient warming. Consequently, we recommend conducting high-level evidence studies to enhance patient recovery by mitigating complications associated with hypothermia during the surgical process.
Acknowledgments: We thank the researchers who conducted this study.
Conflict of Interest: None
Financial Support: None
Ethics Statement: None